
Acquired QT prolongation in a dialysis patient has a long list of potential causes, but most important are electrolyte abnormalities (all the hypo’s: hypokalemia, hypomagnesemia, hypocalcemia) and medications. While significant electrolyte abnormalities are (hopefully) rarely missed, as they’re checked and flagged all the time, it is particularly important to pay attention to medications. A study of the prescription claims of almost 5 million patients found the unacceptably high prescription rates of QT-prolonging medications and dual therapy with two or more QT-prolonging drugs. In fact, 0.5% were taking 5 concomitant QT prolonging agents! The paper included 50 medications that prolong the QT interval and 26 that inhibit their hepatic or renal clearance. The commonest culprits are antibiotics (clarithromycin, erythromycin, levofloxacin) and anti-depressants (fluoxetine, amitriptyline, sertraline, venlafaxine).
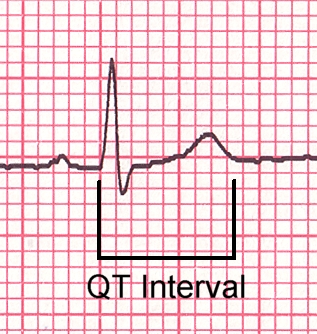
QT interval dispersion (QTd) is less well recognized and often overlooked. QTd, the longest minus the shortest QT interval on a standard ECG, is a marker of variability in ventricular repolarization. A difference of 50 msec or more has been used as a cut-off in several studies (each small box on the ECG is 40ms). QTd is a risk factor for ventricular arrhythmias and sudden death in the general population. It also appearsto be a useful measure to identify dialysis patients at an increased risk for sudden death, based on the following:
- At least 6 studies show that the dialysis procedure is associated with an acute increase in QTd.
- QTd is associated with arrhythmias on Holter monitoring in uremic patients.
- In a Japanese study of 48 ESRD patients, divided into those who did and did not develop increased QTd post-dialysis, there was an increase in cardiac events and cardiac mortality in the group with an increase in QTd postdialysis
- In 147 HD patients followed for up to 9 years, QTd was an independent predictor of total mortality (RR 1.53; P = 0.0001) and cardiovascular mortality (RR = 1.57; P = 0.028) and a trend towards arrhythmia-related mortality (P = 0.06).
Finally, it is worth remembering that QTd may be an epiphenomenon, as it is associated with LVH and structural heart disease, which are themselves strongly associated with sudden cardiac death in ESRD.
No comments:
Post a Comment
Renal Fellow Network encourages comments and discussion regarding the posts. Do not post any comments that are commercial or advertising in nature. Posts will be deleted if commercial or advertising comments are made. Internet users commenting on the Renal Fellow Network must post information which is true and correct to their knowledge. Sources to health/medical claims must be provided when relevant. Moderators reserve the right to erase, without notification, any comment they would judge inappropriate.