
Introduction
About 1 in 6 patient one-liners have Chronic kidney disease (CKD) mixed with a list of comorbidities. It’s easy for a primary care provider (PCP) to forget about the kidneys until it’s too late, or simply pass off the management to a more-than-willing Nephrologist. But knowing the basics of CKD can go a long way for PCPs and some of the new literature can help guide treatment decisions even before getting an office appointment with official bean lovers. As part of the Nephrology Social Media Collective (NSMC) internship I was tasked with writing my first blog post. I decided to tackle a subject bridging my interest with primary care with nephrology. This is a quick rundown of everything a PCP should know about protecting the most important organ.
About 1 in 6 patient one-liners have Chronic kidney disease (CKD) mixed with a list of comorbidities. It’s easy for a primary care provider (PCP) to forget about the kidneys until it’s too late, or simply pass off the management to a more-than-willing Nephrologist. But knowing the basics of CKD can go a long way for PCPs and some of the new literature can help guide treatment decisions even before getting an office appointment with official bean lovers. As part of the Nephrology Social Media Collective (NSMC) internship I was tasked with writing my first blog post. I decided to tackle a subject bridging my interest with primary care with nephrology. This is a quick rundown of everything a PCP should know about protecting the most important organ.
Definition
CKD
is defined as:
1)
The presence of markers of kidney damage for greater than 3 months in blood, urine, or on imaging
a)
e.g proteinuria, non-urological hematuria,
polycystic kidney disease, horseshoe kidney, etc.
OR
2)
The presence of a GFR of less than 60 mL/min/1.73
m2 for more than 3 months
Risk Factors
The
most common cause of
end-stage kidney (ESKD) disease is diabetes (44%), followed by hypertension
(29%). The cause is usually from an increase in
intraglomerular pressure which is damaging to the glomerular filtering capabilities. Other risk factors
include a family history of CKD, autoimmune disease (e.g. SLE, vasculitis,
scleroderma), HIV, Hepatitis B or C, amyloidosis, obstructive nephropathy from
recurrent UTI or nephrolithiasis, and
certain medications (analgesics, immune
suppressants, HIV medications). Acute kidney injuries may also
contribute to CKD, particularly if requiring
inpatient dialysis. Recent evidence suggests pediatric kidney disease
may also be associated with adult ESKD.
Staging and Estimating GFR
Staging
CKD is most frequently done by calculating the estimated glomerular function
rate (eGFR) as a proxy for kidney function. These calculations are often based
on a patient’s serum creatinine (a muscle metabolite that is filtered in the
kidney). Of the three most common calculators (CKD-EPI, MDRD, Cockroft-Gault
equation), the CKD-EPI is the most accurate at predicting
mortality and ESKD and generally is what is recommended for use. (of note- many dose adjustment for drugs still use Cockroft-Gault- look carefully at this when looking at dose adjustments).
After
calculating the eGFR, CKD can be staged into 1 of 5 stages. Using the GFR clock
is one way to remember the eGFR cut-offs for each CKD stage.

Because
the above calculators rely on creatinine (which can vary in patients with
extreme muscle mass e.g. sarcopenic patients such as the frail elderly or
sarco-full patients such as body-builders), creatinine clearance can also be
estimated and used to stage CKD. 24-hour
urine creatinine clearance equation works for all patients regardless of size.
Creatinine clearance is based on the ratio of urine creatinine and plasma
creatinine.
CrCl
= Urine Cr (mg/dl) * Urine volume (ml)] / [Plasma Cr (mg/dl) * Time (min)
Cystatin C is another biomarker that can be used
for estimated eGFR. Like creatinine clearance, it is mostly useful in patients
where creatinine is a bad estimate, though may also help provide more accurate kidney
function estimates when combined with above calculations.
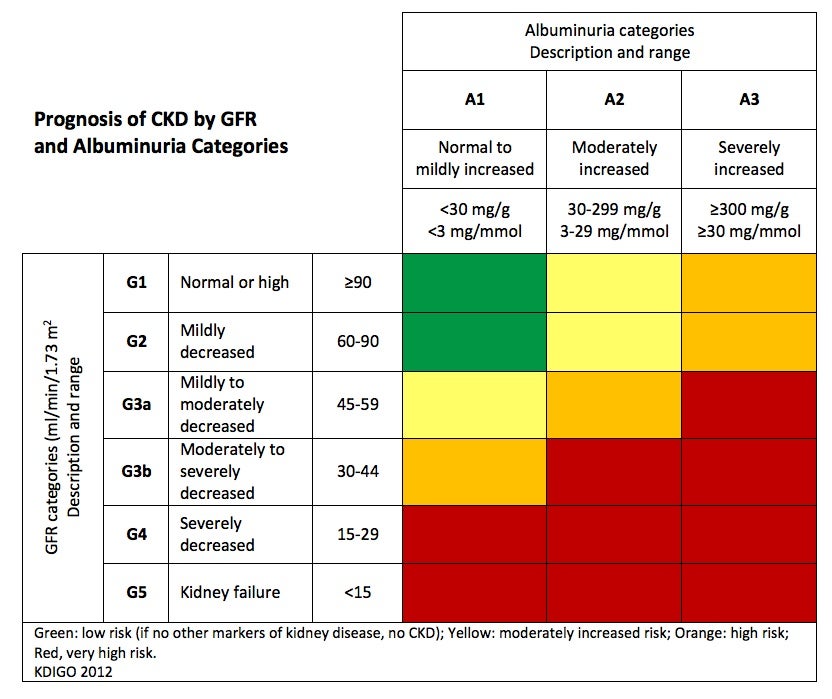
CKD
Staging is also based on the level of proteinuria seen in the patient. If there
is proteinuria or greater than 300mg albumin/mg/g Cr in a urine protein:creatinine
ratio, then the proteinuria is staged as A3. If between 30-300
(microalbuminuria), the staging is A2. A1 is if there is no significant
proteinuria or microalbuminuria.
Prognosis

With
an estimated GFR and knowledge of proteinuria, the risk of kidney failure
requiring dialysis or transplant can be calculated using a Kidney Failure Risk calculator based on Tangri et al, JAMA 2016. More generally,
a lower eGFR has an observed
association with the risk of death, cardiovascular events, and hospitalization.
Initial Work-up
Recommended workup for new
diagnosis of CKD:
●
Serum electrolytes for eGFR and electrolyte
abnormalities (e.g. metabolic acidosis)
●
Complete Blood Cell Count (Anemia)
●
Lipid profile
●
Uric Acid
●
Serum albumin
●
Renal ultrasound
○
to look for hydronephrosis, obstruction, cysts,
stones, and assess kidney size and characterization
●
Urinalysis
○
Quantify proteinuria with urine
protein-to-creatinine ratio (Urine albumin-to-creatinine will miss multiple
myeloma Bence-Jones proteins)
○
Look for hematuria or other signs of glomerulonephritis
●
Consider biopsy if significant proteinuria and no
history of diabetes
In
patients with CKD G3 (eGFR less than 60 mL.min):
●
Serum calcium, phosphorus, PTH, Vitamin D to
assess for Bone Mineral Disease
If
suggested by the history and physical examination and UA:
●
Antinuclear antibody testing to evaluate for
lupus
●
Hepatitis B and C, and HIV serology
●
Serum antineutrophil cytoplasmic antibodies to
evaluate for ANCA-associated vasculitis
●
Serum and urine protein immunoelectrophoresis to
test for multiple myeloma
Monitoring
All
patients with at least CKD G4 disease (GFR ≤30 mL/min/1.73 m2 )
should establish care with a nephrologist. Consultation is also
recommended if proteinuria greater than 3g / 24 hr, evidence of
glomerulonephritis (hematuria, proteinuria, and hypertension), an eGFR decline
of 50% within 1 year.
General
management should also prioritize treatment of the underlying condition (e.g.
hypertension and diabetes) to reverse the progression of CKD.
Management
Medications
ACE-inhibitors
demonstrate a significant reduction in progression of CKD and reduction in
proteinuria per the RENAAL, IDNT, and other trials. Fewer patients
had progression to ESKD though a mortality benefit was not observed.
Of
note, ACE-inhibitors or ARBs (RAAS blockade) are likely to cause a benign increase in serum
creatinine. In general, if the creatinine bump greater than 30%, RAAS blockade should be discontinued. An increase in creatinine after ACE-I may show greatest risk of mortality (though it is
unclear what would happen if the patients with bumps were not on ACE-I, so this
is not an indication to necessarily discontinue therapy).
Blood
Pressure Treatment
Per
KDOQI 2012 guidelines, target
blood pressure in CKD is less than 130 over 80 mm Hg. With<130 mmhg.="" span="" style="mso-spacerun: yes;"> <130 mmhg.="" nbsp="" span="">ACE-inhibitors being the first
line drug.
Diabetes
Control
Metformin: if eGFR 30-45 and already on metformin (and this is not AKI) can continue metformin. Do not start NEW if eGFR is 30-45, but ok if higher than 45.
SGLT2 inhibitors
(i.e. Empagliflozin and Canagliflozin) are associated with lower rates of
worsening nephropathy, progression to macroalbuminuria, initiation of renal
replacement therapy and mortality. (EMPA-Reg, EMPA-Reg ESRD + CANVAS). However, studies demonstrating their effectiveness in CKD are ongoing.
Bone
Mineral Disease Screening
All
patients with CKD G4 should be screened for secondary and tertiary
hyperparathyroidism. The screening labs are a PTH,
phosphorus, calcium and vitamin D level. Further information can be found at
the KDIGO guidelines on BMD.
Depression
Screening
Anemia
There
are multiple causes of anemia in patients with CKD including iron
deficiency. KDIGO
recommends intravenous iron for anemic, nondialysis, CKD patients with
transferrin saturation
<30 and="" ferritin="" isual="" span="" summary="">here).
Nutrition
Guidelines remain
controversial but a full discussion can be found at the AKJD Blog
or in the recent NEJM Review.
Medications
to Avoid
Bactrim
Use
of Bactrim (trimethoprim-sulfamethoxazole) was associated with 3 excess cardiac deaths per
1,000 prescriptions presumably due to hyperkalemia (e.g. patients with CKD are higher risk)
Baclofen- should be avoided in ESKD or eGFR less than 30 and dose reduced with eGFR between 30-6o.<30 .="" 30-60="" adjustment.="" dose="" font="" requires="">
Baclofen- should be avoided in ESKD or eGFR less than 30 and dose reduced with eGFR between 30-6o.<30 .="" 30-60="" adjustment.="" dose="" font="" requires="">
Proton Pump Inhibtors
Renally dosed medications
Contrast?
Contrast-induced
kidney injury (CIN) may be overestimated in literature. The AMACING trial shows that
pre-hydration does not reduce kidney injury in those exposed to contrast.
NSAIDS?
Patients
with CKD depend on prostaglandins for vasodilation of afferent
arterioles and renal blood flow. NSAIDs block prostaglandin activity and
can cause acute kidney injury. KDIGO
Guidelines recommend avoiding NSAIDS in patients with CKD, but the evidence
suggests that risk of NSAID use in CKD patients is pretty low: The Male Physician Study showed no
elevation in serum creatinine with consistent NSAID use. However, the PRECISION Trial showed only ~1%
risk of kidney events in CKD patients with daily high-dose NSAIDs.
For a more succinct review of the above, check out the new ClinicWiki page on Chronic Kidney Disease.
Post written by
Justin Berk, MD, MPH @justinberk
Med-Peds Resident, John
Hopkins University
NSMC Intern 2018














{kind=link}
No comments:
Post a Comment