
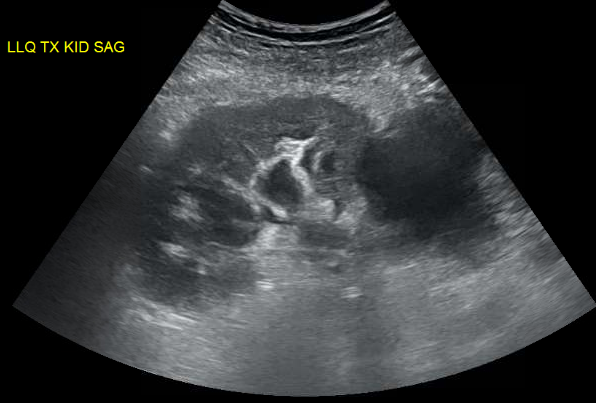
We were evaluating a kidney transplant recipient three weeks after surgery who presented with a rise in creatinine. We obtained an ultrasound which showed a large fluid collection and mild hydronephrosis. Prograf level was at goal.
Peritransplant fluid collections may be produced by lymphoceles, urinomas, hematomas or abcesses. These collections may compress the ureter leading to hydronephrosis or may compress the renal vein causing a “compartment-like syndrome”. Since his creatinine was risen, we decided to drain the fluid collection. An important point is that mild hydronephrosis is reported in a large portion of kidney transplant ultrasounds and intervention is usually driven by the clinical setting. When in doubt, serial ultrasounds indicating progressive dilatation or the use of nuclear medicine imaging showing normal perfusion and parenchymal uptake but pooling of tracer in the renal pelvis with prolonged pelvic retention helps in confirming the diagnosis.
His INR was 2.1 due to coumadin for a history of multiple clotted fistula. The interventional radiologist requested that we give FFP to reduce his INR to below 1.5 before considering the procedure. It was late Friday so we got 4U of FFP in and repeated INR. We were hoping that 4U of FFP would quickly reverse his mildly elevated INR.
Interestingly, data supporting that is lacking.
FFP can have an INR as high as 1.5 and transfusion of FFP will have little effect on minimally elevated INRs (Gearoid actually pointed that out in rounds). A study of the use of FFP in 121 patients with an INR in the range of 1.1 to 1.85, showed that correction of the INR to normal was achieved in only one patient (0.8 percent) and correction at least halfway to normal in only 15 percent. The median decrease in the PT and INR was 0.2 seconds and 0.07, respectively, and was independent of the number of units of FFP infused (median 2 units; range 1 to 20). Thus, available studies do not support the efficacy of FFP in treating bleeding or as prophylaxis for invasive procedures in patients with a mild coagulopathy (ie, INR below 2.0).
After some discussion with IR, they agreed to go ahead with the procedure with an INR 1.9. About 600cc of yellow fluid was drained. Fluid creatinine was checked and was similar to serum level, ruling out an urinoma. This patient’s fluid collection was a lymphocele, which is the most common cause of peritransplant fluid collection due to disruption of renal lymphatics. It usually occurs weeks after surgery and drainage is required only in cases of suspected obstruction. With time, the amount of fluid collection tends to subside. Soon after drainage, his creatinine started to come down confirming the cause of his worsening renal function.
Figure: large peri-transplant fluid collection with associated hydronephrosis.














1 comment:
I am glad someone is finally pointing out the uselessness of FFPs in slightly elevated INRs.
Same thing with liver patients, there was an interesting lecture by Dr Dzik from MGH transfusion medicine stating that liver patients with an INR of up to 1.8 can have normal clotting (both pro and anticoagulants are reduced but the balance is the same therefore normal clotting).
Maybe the intentions of the clinician to have his patient have "Harvard labs" are good but not always supported by evidence.
Post a Comment