
In 2015 I hope to blog on articles from non-renal journals that are of interest to nephrologists. First
up is cardiology and a topic that has been covered in previous RFN posts (here, here, here). The optimal
management of atrial fibrillation in patients with CKD is controversial as they are at both a higher
risk of stroke and higher risk of bleeding than the non-CKD population; this is particularly true of
patents on dialysis. Warfarin is well established in reducing the risk of stroke in patients with atrial
fibrillation but the trials excluded patients with a creatinine clearance of < 30ml/min. Thus we have
had to rely on, often contradictory, observational studies to guide us in this area.
A study in the Journal of the American College of Cardiology in December is the latest to
investigate the net clinical benefit (or harm) of antithrombotic therapy in these patients. It was a
retrospective cohort study using nationwide Danish registries to identify all patients discharged from
hospital with a diagnosis of non-valvular AF between 1997 to 2011. Out of the 154,259 patients
identified; 11,128 (7.2%) had non-end stage CKD and 1,728 (1.1%) were receiving dialysis. They used
the CHA2DS2-VASC score to stratify the patients into high and low/intermediate risk of stroke groups.
Briefly the score is calculated by adding one point for heart failure, hypertension, diabetes, vascular
disease, age 65-74 and female sex and 2 points for age over 75 and a previous stroke. A score of ≥ 2
is considered high risk.
They found that among high risk patients on dialysis, warfarin was associated with a significantly
lower risk of all-cause mortality (HR 0.85, CI 0.72-0.99) and there was a non-significant trend toward
a reduction in cardiovascular death and a composite end point of hospitalization or death from all
stroke/all bleeding. There was no benefit of warfarin in low-intermediate risk dialysis patients; indeed
there was a trend toward higher all-cause mortality (HR 1.36, CI 0.96-1.94).
Analysis of a sample of the non-end stage CKD patients found 19.1% were CKD stage 1-2, 20% were
CKD 3, 36.4% were CKD 4 and 24.5% were CKD 5. Warfarin was associated with significantly lower
risk of all-cause mortality in both high risk (HR 0.64) and low-intermediate risk groups (HR 0.62) in
patients with non-end stage CKD. One caveat, highlighted in the journal’s editorial, is that certain
components of the CHA2DS2-VASC score (diabetes, hypertension and heart failure) were identified
based on filled prescription data, meaning the frequency of these risk factors may have been
underestimated and therefore overestimating the number of patients classified as low-intermediate
risk. We should therefore interpret the mortality benefit for this group with caution.
The most recent NICE guidelines in the UK, published in June 2014, do not recommend aspirin as
monotherapy for the prevention of stroke in patients with AF. This study suggests the same should
apply to patients on dialysis as aspirin was not associated with a lower risk of any outcome.
Analysis of the newer anticoagulants such as Dabigatran, Rivaroxaban and Apixaban, were not
included in this study. They are contraindicated in patients with ESRD as they are cleared via the
kidneys and drugs levels can accumulate and precipitate bleeding though their use in this setting has
increased nonetheless. A study from the U.S. out this month in Circulation found that 5.9% of
anticoagulated patients with AF on dialysis are started on dabigatran or rivaroxaban and that these
drugs were associated with a higher risk of hospitalisation or death from bleeding compared to
warfarin.
Balancing the risks and benefits of anticoagulation in patients with AF and ESRD remains complex.
The current evidence suggests that warfarin remains the best anti-thrombotic available but it also
has a significant potential for harm and the decision of whether or not to start treatment needs to
be an individualized patient choice.
Authored by David Baird
Royal Infirmary of Edinburgh
Showing posts with label Anticoagulation. Show all posts
Showing posts with label Anticoagulation. Show all posts
Tuesday, February 3, 2015
Sunday, January 26, 2014
Warfarin for Atrial Fibrillation in Dialysis Patients: Where’s the data?

A current study from Canada in Circulation weighs in on the issue. The authors conducted a retrospective cohort study of patients > 65 years admitted with a diagnosis of AF from 1998 to 2007. There were 1,626 dialysis patients (46% received warfarin) and >200,000 non-dialysis patients. In a multivariate analysis, warfarin use in the dialysis patients was associated with similar risk of non-hemorrhagic stroke but a significantly higher risk of bleeding (defined as intra-cerebral, intra-ocular, GI, unspecified hemorrhage & hematuria; HR 1.44). The non-dialysis patients did see a lower incidence of ischemic stroke with warfarin use.
Our ESRD patients comprise a unique cohort with labile, often high blood pressure, repetitive AV access puncture, proven variability in INR and usually anticoagulation use during dialysis. They are certainly high risk for bleeding. Moreover, warfarin use is associated with accelerated vascular calcification in CKD patients and calciphylaxis, an admittedly uncommon but devastating condition. Unfortunately we suffer from a lack of alternatives to warfarin. Accumulation of low-molecular weight heparin in ESRD precludes its use and there is no experience with newer agents such as direct thrombin and Factor Xa inhibitors.
Many authors, including those at UpToDate, recommend warfarin use with AF and an eGFR<15mls/min. They are equivocal when CHADS2=0, but this is rare in a dialysis patient. Remember CHADS2 includes congestive heart failure, hypertension, age ≥75, diabetes and previous stroke/TIA. Despite older age being part of the CHADS2 score suggesting treatment efficacy, age >75 has been associated with a particularly high risk of bleeding in dialysis patients treated with warfarin. Also, CKD is part of the HAS-BLEED score which predicts high risk of hemorrhagic complications to warfarin when the score is ≥3. Many dialysis patients would fall into this category based on hypertension, older age and concomitant meds (85% in the current study in Circulation). I often feel uncomfortable using warfarin in ESRD and certainly feel it should be an individualized patient choice. With the current evidence (or lack of it) to guide us and the significant potential for harm, withholding warfarin for many of our older dialysis patients would not seem unreasonable.
Sunday, September 8, 2013
Thromboembolic Prophylaxis in Patients with AFib and CKD: Caught between the Devil and the Deep Blue Sea
I often get curb-sided by cardiologists and internists for
my opinion on using warfarin or other anticoagulants for thromboembolic risk
prophylaxis in CKD +/- Afib patients. A similar conundrum of using
anticoagulation for stroke prophylaxis in dialysis patients was discussed about
three
years ago on this blog by Conall. Like many other issues in patients with
CKD, things are not always black-and-white, and a lot could depend on patient
and physician preference. This often
makes the “right answer” a confusing exercise, since CKD patients are also at a
higher bleeding risk. Most randomized trials addressing this issue have
excluded patients with a GFR below 30. Furthermore, newer direct thrombin
inhibitors (dabigatran), or Factor Xa inhibitors
(apixaban, rivaroxaban) are available, which might be better than warfarin, at
least in the early-CKD patient (although the lack of a reversing antidote is a
potential pitfall). Finally, warfarin has a well-established link with vascular
calcification (a mortality risk) in dialysis patients. As nephrologists, it is
imperative that we are knowledgeable about the best-available data that can
help us make an evidence-based recommendation, and so I put together a concise
decision-table with links to primary literature sources.
In addition to the “traditional” risk factors for stroke in
patients with AFib (as exemplified by the acronym CHADS), it is known that CKD itself
is an independent risk factor for stroke. Thus CKD patients, both with, and without
AFib, are at an increased risk of stroke. This has been demonstrated in CKD as well as dialysis patients, and the risk
worsens with decline in GFR.
Thus, with the above background in mind, the two main
variables that determine what, if any, anticoagulation is to be used in this
setting, are (1) the stage of CKD, and (2) the CHADS2 score:
|
CHADS2 Score
|
CKD STAGE
|
||
|
Stage 3, eGFR 30-59
|
Stage 4, eGFR 15-29
|
Stage 5, eGFR less than 15, or dialysis
|
|
|
0
|
|
|
|
|
>1
|
AC (Direct thrombin inhibitors (dabigatran), and
Factor Xa inhibitors (rivaroxaban, apixaban)
potentially superior to warfarin
|
AC (warfarin preferred since no data on direct thrombin
or factor
Xa inhibitors)
|
AC (warfarin preferred since no data on direct thrombin
or factor
Xa inhibitors)
|
ASA = Aspirin
AC = Anticoagulation
?? = Expert opinion only, no strong evidence available - weight risks vs. benefits
Remember that no antithrombotic therapy is warranted if bleeding is a concern
Posted by Veeraish Chuahan
(Apologies for any formatting issues)
Sunday, May 6, 2012
Diagnosis and Management of Post-Transplant Fluid Collections
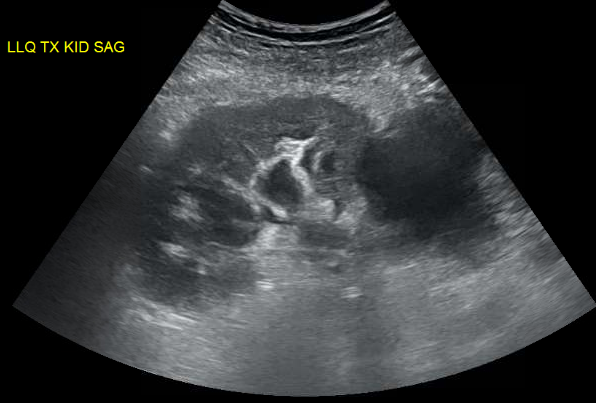
We were evaluating a kidney transplant recipient three weeks after surgery who presented with a rise in creatinine. We obtained an ultrasound which showed a large fluid collection and mild hydronephrosis. Prograf level was at goal.
Peritransplant fluid collections may be produced by lymphoceles, urinomas, hematomas or abcesses. These collections may compress the ureter leading to hydronephrosis or may compress the renal vein causing a “compartment-like syndrome”. Since his creatinine was risen, we decided to drain the fluid collection. An important point is that mild hydronephrosis is reported in a large portion of kidney transplant ultrasounds and intervention is usually driven by the clinical setting. When in doubt, serial ultrasounds indicating progressive dilatation or the use of nuclear medicine imaging showing normal perfusion and parenchymal uptake but pooling of tracer in the renal pelvis with prolonged pelvic retention helps in confirming the diagnosis.
His INR was 2.1 due to coumadin for a history of multiple clotted fistula. The interventional radiologist requested that we give FFP to reduce his INR to below 1.5 before considering the procedure. It was late Friday so we got 4U of FFP in and repeated INR. We were hoping that 4U of FFP would quickly reverse his mildly elevated INR.
Interestingly, data supporting that is lacking.
FFP can have an INR as high as 1.5 and transfusion of FFP will have little effect on minimally elevated INRs (Gearoid actually pointed that out in rounds). A study of the use of FFP in 121 patients with an INR in the range of 1.1 to 1.85, showed that correction of the INR to normal was achieved in only one patient (0.8 percent) and correction at least halfway to normal in only 15 percent. The median decrease in the PT and INR was 0.2 seconds and 0.07, respectively, and was independent of the number of units of FFP infused (median 2 units; range 1 to 20). Thus, available studies do not support the efficacy of FFP in treating bleeding or as prophylaxis for invasive procedures in patients with a mild coagulopathy (ie, INR below 2.0).
After some discussion with IR, they agreed to go ahead with the procedure with an INR 1.9. About 600cc of yellow fluid was drained. Fluid creatinine was checked and was similar to serum level, ruling out an urinoma. This patient’s fluid collection was a lymphocele, which is the most common cause of peritransplant fluid collection due to disruption of renal lymphatics. It usually occurs weeks after surgery and drainage is required only in cases of suspected obstruction. With time, the amount of fluid collection tends to subside. Soon after drainage, his creatinine started to come down confirming the cause of his worsening renal function.
Figure: large peri-transplant fluid collection with associated hydronephrosis.
Friday, March 2, 2012
Handling anticoagulation peri-kidney biopsy

Kidney biopsy is considered the most invasive procedure nephrologists are involved. Though complication rates are small, bleeding requiring surgery has been reported to occur in 1 in 1,000 kidney biopsies. More commonly, patients may develop a decrease in hemoglobin by 1 point (~50% of cases) and/or gross hematuria (3-18%). The risk of bleeding complications become much higher in patients that require peri-biopsy anticoagulation.
A new evidence-based guideline was just published on Chest 2012, summarizing the best approach to anticoagulation in a number of different scenarios. Overall, the new recommendations are more conservative than before regarding anticoagulation peri-procedure.
To illustrate that, let’s use a theoretical patient on anticoagulation with coumadin (6mg daily) due to Factor of V Leiden mutation and prior history of thrombosis (more than 6mo ago).
In preparation for the procedure, the physician would recommend stopping coumadin 5 days prior to the kidney biopsy and bridging with either UFH or LMWH. This is usually started on day 3 prior to the procedure. The major difference in approach now is related to when should the bridging anticoagulation be stopped and restarted. The novel guidelines recommend the following:
* If on IV heparin, stop infusion 4-6 hours prior to procedure
* If on LMW, last dose should be 24 hours prior to procedure (rather than 12 hours before)
* Resuming coumadin should occur 12-24 hours after procedure if no evidence of bleeding
* Bridging anticoagulation with LMWH or UFH should be restarted 48-72 hours after the procedure (rather than 24 hours after surgery). Since most of the bleeding after kidney biopsy will occur in the first 24 hours, I believe delaying for another 24 hours would only be warrant in major surgeries with higher bleeding risks)
Most of these recommendations are grade 2C (weak), therefore individual interpretation is warranted.
My take-home summary of anticoagulation peri-kidney biopsy in high risk patients for thromboembolism would be:
Stop coumadin 5 days before procedure; admit the patient with renal failure 3 days prior to biopsy for bridging with UFH; stop UFH at least 4 hours prior to procedure; resume coumadin/UFH 6-24 hours after bx if no evidence of bleeding (stable Hb, vital signs and no significant hematuria).
Though this is a general suggested approach, remember to assess the thromboembolic risk for each individual patient before proceeding with a kidney biopsy. As an example, I would favor restarting anticoagulation much earlier after bx in a patient with history of multiple clots (6 hours after biopsy).
Below additional general recommendations about anticoagulants from the new guidelines:
- Dosing of UFH: 80U/kg bolus followed by 18U/kg/hour
- Dosing of coumadin: loading with 10mg daily for first 2 days [[personal opinion: this loading dose may be too high for elderly or cachetic patients]]
- Dosing of enoxaparin: 1mg/kg BID; if GFRb below 30 ml/min: 1mg/kg daily
- Dosing of fondaperinox: 5mg daily if less than 50kg; 7.5mg if 50-100kg and 10mg if more than 100kg. Avoid if GFR less than 30 ml/min.
- Dosing of dalterapin : 200 U/kg daily. Accumulation expected in renal failure but no specific dose adjustment has been recommended, so should likely be avoided until trials available.
- Despite recent publications about benefits of genotyping in predicting response to coumadin, the guidelines recommend against this practice.
Thursday, March 31, 2011
Argatroban

A nticoagulant of choice in active HIT-II or HITT.
R enal dose adjustment not necessary – hepatically cleared only.
G oal aPTT is 2-3 times above baseline (as for heparin).
A ctivated PTT is monitoring test of choice, but note argatroban increases ACT and PT/INR also.
T wo mcg per kg per minute is the usual starting dose (2mcg/kg/min)
R eversal not possible, so careful monitoring essential.
O .5 mcg/kg/min starting dose in liver disease (0.5mcg/kg/min)
B olus not required before infusion (unlike heparin). Steady state within 3 hours.
A lbumin: Low albumin is an important clue to hepatic synthetic dysfunction. Reduce starting dose by 75% if present.
N ormalised ratio: When transitioning to warfarin, once the INR is 4 while on both drugs, the INR will be therapeutic once the argatroban infusion is stopped. The alternative is the measure the chromogenic factor x level (goal less than 45% for efficacy).
Subscribe to:
Comments (Atom)













