
Helen, 37, is single and works full-time as a teacher. She is very keen to be a kidney donor to her loved one. You measure her BP at 140/85. Her BMI is 28kg/m2. Her physical examination and urinalysis are unremarkable. Talking to Helen, you establish a family history of hypertension and type 2 diabetes in her older relatives, and learn that she does not plan on becoming pregnant in the future.
Pending completion of investigations, you believe:
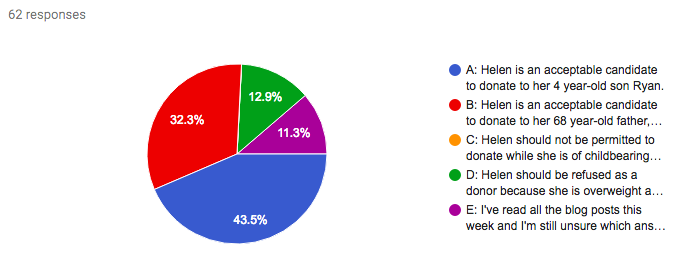
A) Helen is an acceptable candidate to donate to her 4 year-old son Ryan.
B) Helen is an acceptable candidate to donate to her 68 year-old father, Bert, who has diabetes and is on dialysis.
C) Helen must not be permitted to donate while she is of childbearing age.
D) Helen should be refused as a donor because she is overweight and has a family history of both diabetes and hypertension.
E) I've read all the blog posts this week and I'm still unsure which answer to choose.

Here's how you responded:
Now, before you make a formal complaint, you’re absolutely right: this question would not hold water as a standardized board-level MCQ! There’s more than one correct answer. It’s controversial. And it’s perhaps not a direct test of the knowledge you’ve worked to acquire over the course of Living Kidney Donor Case Challenge.
However, every response from A through D is a real-life comment from a real-life nephrologist in an equivalent clinical scenario. So the range of responses from our #LKDCC community is not at all surprising. And if you chose E, don’t worry!
By following the whole week of #LKDCC, you’ve gained an insight into the available evidence regarding risks to kidney donor candidates. You’ve learnt about the risks of ESKD, proteinuria and pre-eclampsia. You’ve pondered the potential contribution of body composition, ethnic background, family history, dysglycaemia and age to these risks. You can confidently explain the ‘known knowns’ to would-be kidney donors. And hopefully you recognise the ‘known unknowns’ as well: the current gaps in evidence that are equally important to discuss with donors, but partly explain why there is such diversity between nephrologist attitudes in this field. We all - doctors and patients - weigh unquantifiable risk differently: some are more conservative, others more adventurous.
So what does this mean for Helen? Helen is a motivated donor candidate with some risk factors for future metabolic and cardiovascular disease, including elevated BMI and family history. It’s essential that these are addressed in the informed consent process as we counsel Helen. We should explain to Helen how lifestyle choices could reduce her future risk of diabetes, discussing the benefits of weight loss and physical activity. She is of childbearing age, and therefore our consultation should also take into account her reproductive history and the potential impact of donation on any future pregnancy.
Is it important to us, as Helen’s medical advocate, who the intended recipient is? Arguably, it is not, except perhaps to establish that Helen’s relationship with the recipient is not complicated by coercion or exploitation. Our role is to assess Helen’s medical suitability as a donor, and to ensure she understands the implications of donation. As a mother who performs peritoneal dialysis for her son every day, and wishes for a long healthy life for him, Helen brings an understandably strong motivation for donation. As a donor to her father, Helen may be aware of the potentially shorter lifespan of the donated organ, but remain motivated to relieve her father of the burden of haemodialysis, thereby improving his survival and quality of life, and, by extension, her quality of life as a daughter and carer. Given the choice, as resource allocators, we would prefer to see Helen's kidney give benefit to a younger recipient - perhaps that explains why 43.5% of the #LKDCC team chose Option A. Similarly, if there were an alternative choice of donor, such as Helen's mother, whose lifetime risk may be lower than 37 year-old Helen, that risk differential should be clearly outlined in counselling Helen and her family. Ultimately, when it comes to risk-benefit analysis in living kidney donation, there are no measurable medical benefits. The potential benefits are all psychosocial, and therefore only truly definable by each individual donor, after thorough counselling.
Living kidney donors don’t need paternalistic protection from unquantifiable long-term risks. They need our guidance, in providing them with all the available information to make a reasoned decision, while continuing the research required to expand the evidence base. They need our advocacy, firmly representing their individual needs in the multi-pronged transplant process. And they need our support to undertake a risk-benefit analysis that is truly unique across all of medicine.
Thank you for participating in #LKDCC: please give us your feedback here
Now you'll have a whole new perspective on Living Kidney Donor Risk
and the #NephMadness #TransplantRegion
Don't forget to submit your #NephMadness brackets here
Now you'll have a whole new perspective on Living Kidney Donor Risk
and the #NephMadness #TransplantRegion
Don't forget to submit your #NephMadness brackets here
Please note these are fictional cases with open access stock images. They do not represent real cases.
Created by Kate Robson (Nephrologist, Melbourne, Australia and NSMC Intern 2018)














No comments:
Post a Comment